|
Overview
During contraction of the calf muscle, tension is placed through the Achilles tendon and this rubs against the retrocalcaneal bursa. Compressive forces and friction may also be placed on the retrocalcaneal bursa during certain ankle movements or by wearing excessively tight shoes. When these forces are excessive due to too much repetition or high force, irritation and inflammation of the bursa may occur. This condition is known as retrocalcaneal bursitis. Causes Wearing poorly fitting or constrictive footwear can cause the heel to become irritated and inflamed. Shoes that dig into the back of the heel are the primary cause of retroachilles bursitis. Foot or ankle deformity. A foot or ankle deformity can make it more likely to develop retrocalcaneal bursitis. For example, some people can have an abnormal, prominent shape of the top of their heel, known as a Haglund's deformity. This condition increases the chances of irritating the bursa. A trauma to the affected heel, such as inadvertently striking the back of the heel against a hard object, can cause the bursa to fill with fluid, which in turn can irritate and inflame the bursa's synovial membrane. Even though the body usually reabsorbs the fluid, the membrane may stay inflamed, causing bursitis symptoms. Symptoms Symptoms of Achilles bursitis are often mistaken for Achilles tendinitis because of the location of the pain at the back of the heel. When you suffer from Achilles bursitis you will experience some or all of the following symptoms which are most noticeable when you begin activity after resting. High heels can add pressure on the retrocalcaneal bursa, subcutaneous calcaneal bursa, and Achilles tendon. Diagnosis Plain radiographs of the calcaneus may reveal a Haglund deformity (increased prominence of the posterosuperior aspect of the calcaneus). However, on weight-bearing lateral radiographs, the retrocalcaneal recess often appears normal even in patients with retrocalcaneal bursitis, limiting its usefulness in making this diagnosis.Radiographs may be used as a diagnostic measure to support a clinician?s diagnosis of retrocalcaneal bursitis. Individuals with retrocalcaneal bursitis may have an absence of the normal radiolucency (ie, blunting) that is seen in the posteroinferior corner of the Kager fat pad, known as the retrocalcaneal recess or bursal wedge. This may occur with or without an associated erosion of the calcaneus. Non Surgical Treatment All types of bursitis often can be successfully managed non-surgically, and possible treatments include use of ice packs or compressive dressings, activity modification that may reduce stress or irritation, administration of nonsteroidal anti-inflammatory drugs (NSAIDs) or antibiotics, corticosteroid injections (knee and elbow), stretching exercises, and/or change of footwear (heel). Surgery may be required in patients whose symptoms remain following these treatments and in certain situations when infection is involved. Surgical Treatment Surgery is rarely need to treat most of these conditions. A patient with a soft tissue rheumatic syndrome may need surgery, however, if problems persist and other treatment methods do not help symptoms.  Overview OverviewA Hammer toes is the result of deformed toe joints, tight tendons that attach to the toe, and misaligned toe bones. The usual appearance of a hammertoe is a toe bent upward at the middle toe joint, so that the top of this joint rubs against the top of the shoe. The remainder of the toe is bent downward so that, instead of the entire toe bearing weight, only the tip of the toe bears weight. Pain can occur on the top of the toe, the tip of the toe, or in both areas. Causes Hammertoes are most common in women, and a big part of this is poor shoe choices, which are a big factor in the development of many foot problems. Tight toe boxes and high heels are the biggest culprits. Genetics certainly plays a role in some cases of hammertoes, as does trauma, infection, arthritis, and certain neurological and muscle disorders. But most cases of contracted toes are associated with various biomechanical abnormalities in how a patient walks. This causes the muscles and tendons to be used excessively or improperly, which deforms the toes over time.  Symptoms SymptomsPeople with a hammer toe will often find that a corn or callus will develop on the top of the toe, where it rubs against the top of the footwear. This can be painful when pressure is applied or when anything Hammer toe rubs on it. The affected joint may also be painful and appear swollen. Diagnosis Hammer toes may be easily detected through observation. The malformation of the person's toes begin as mild distortions, yet may worsen over time - especially if the factors causing the hammer toes are not eased or removed. If the condition is paid attention to early enough, the person's toes may not be permanently damaged and may be treated without having to receive surgical intervention. If the person's toes remain untreated for too long, however the muscles within the toes might stiffen even more and will require invasive procedures to correct the deformity. Non Surgical Treatment Hammertoes that are not painful (asymptomatic) and still flexible may not require treatment. In mild cases, open-toed, low-heeled, or wider shoes and foam or moleskin pads can provide symptomatic relief by reducing pressure. Taping (strapping) the affected toe can help to reduce deformity and pain. Physical therapy to instruct patients in exercises that passively stretch tight structures and strengthen weak foot intrinsic muscles is also helpful with mild cases. Periodic trimming (debridement) of corns (clavi, helomata) by a podiatrist can provide temporary relief. Corticosteroid injections are often very effective in reducing pain. Surgical Treatment Surgical correction is necessary in more severe cases and may consist of removing a bone spur (exostectomy) removing the enlarged bone and straightening the toe (arthroplasty), sometimes with internal fixation using a pin to realign the toe; shortening a long metatarsal bone (osteotomy) fusing the toe joint and then straightening the toe (arthrodesis) or simple tendon lengthening and capsule release in milder, flexible hammertoes (tenotomy and capsulotomy). The procedure chosen depends in part on how flexible the hammertoe is.
Overview
 Bunions are bony bumps that form on the side of the big toe joint or baby toe joint (these are commonly called ?bunionettes? or ?tailor?s bunions?). Bunions most commonly result from one or more of the following factors: genetics, faulty foot mechanics like over-pronation, and/or long periods of time spent in improperly fitting footwear. Bunions can start with audible clicking (called ?crepitus?) and/or stiffness in the affected joint which indicates that the joint surfaces are rubbing together improperly. This may progress to include inflammation, degeneration of the surfaces of the joint, deformity (including bone growth at the joint line and displacement of the toe) and ultimately, loss of range of motion in the joint. Bunions are bony bumps that form on the side of the big toe joint or baby toe joint (these are commonly called ?bunionettes? or ?tailor?s bunions?). Bunions most commonly result from one or more of the following factors: genetics, faulty foot mechanics like over-pronation, and/or long periods of time spent in improperly fitting footwear. Bunions can start with audible clicking (called ?crepitus?) and/or stiffness in the affected joint which indicates that the joint surfaces are rubbing together improperly. This may progress to include inflammation, degeneration of the surfaces of the joint, deformity (including bone growth at the joint line and displacement of the toe) and ultimately, loss of range of motion in the joint.Causes The main cause of bunions is excessive pressure being placed on the front of the foot, and is usually the result of wearing high-heeled shoes with pointed toes. A study by the American Orthopaedic Foot and Ankle Society found that 88 percent of women in the United States wear shoes that are too small and that 55 percent of them have bunions. Overall, bunions are nine times more common in women than men. In some cases, bunions are hereditary; they also may be caused by arthritis or polio. Symptoms Red, thickened skin along the inside edge of the big toe. A bony bump at this site. Pain over the joint, which pressure from shoes makes worse. Big toe turned toward the other toes and may cross over the second toe. Diagnosis The doctor considers a bunion as a possible diagnosis when noting the symptoms described above. The anatomy of the foot, including joint and foot function, is assessed during the examination. Radiographs (X-ray films) of the foot can be helpful to determine the integrity of the joints of the foot and to screen for underlying conditions, such as arthritis or gout. X-ray films are an excellent method of calculating the alignment of the toes when taken in a standing position. Non Surgical Treatment Your podiatrist can recommend exercises, orthoses (special devices inserted into shoes), shoe alterations or night splints (which hold toes straight over night) which may slow the progression of bunions in children. According to experts, ?conservative? measures such as these may help relieve symptoms, though there is no evidence they can correct the underlying deformity. Orthoses are designed to prevent the problem getting worse by decreasing any biomechanical causes of bunions. In other words, if the biomechanical theory is correct (i.e. if your bunions are caused by the way you walk), orthoses may help you walk in a way that doesn?t exacerbate the problem. But it won?t change the already established shape of your foot. For that, you need surgery.  Surgical Treatment If conservative treatment doesn't provide relief from your symptoms, you may need surgery. The goal of bunion surgery is to relieve discomfort by returning your toe to the correct position. There are a number of surgical procedures for bunions, and no one technique is best for every problem. Surgical procedures for bunions might involve removing the swollen tissue from around your big toe joint. Straightening your big toe by removing part of the bone. Realigning the long bone between the back part of your foot and your big toe, to straighten out the abnormal angle in your big toe joint. Joining the bones of your affected joint permanently. It's possible you may be able to walk on your foot immediately after a bunion procedure. However, full recovery can take weeks to months. To prevent a recurrence, you'll need to wear proper shoes after recovery. It's unlikely that you'll be able to wear narrower shoes after surgery. Surgery isn't recommended unless a bunion causes you frequent pain or interferes with your daily activities. Talk to your doctor about what you can expect after bunion surgery. Prevention Because bunions develop slowly, taking care of your feet during childhood and early adulthood can pay off later in life. Keep track of the shape of your feet as they develop over time, especially if foot problems run in your family. Exercising your feet can strengthen them. Learn to pick up small objects, like a pencil or pebble, with your toes. Wear shoes that fit properly and don't cramp or pinch your toes. Women should avoid shoes with very high heels or pointed toes. Overview
The problem with pronation is when it is excessive, here the term overpronation (or hyper-pronation) is used. This is quite a common problem and can lead to a number of injuries, especially in runners, including shin splints, anterior compartment syndrome, patello-femoral pain syndrome, plantar fasciitis, tarsal tunnel syndrome, bunions (Hallux valgus) and achilles tendonitis.  Causes Over-pronation occurs when the foot collapses too far inward stressing the plantar fascia (the area underneath the arch of the foot.) Normally, one pronates every time he or she walks, but excessive pronation is called over-pronation. When this occurs it can cause pain in the feet, knees, hips, low back and even the shoulder. Decreasing over-pronation, which is very prominent in runners, will help add endurance, speed and efficiency to your run and ultimately place less stress on your body. Symptoms Due to the laxity of the soft tissue structures of the foot, and the fact that the joints are not held together properly, the bones of the feet shift. When this occurs, the muscles that attach to these bones must also shift, or twist, in order to attach to these bones. The strongest and most important muscles that attach to our foot bones come from our lower leg. So, as these muscles course down the leg and across the ankle, they must twist to maintain their proper attachments in the foot. This twisting of these muscles will cause shin splints, Achilles Tendonitis, generalized tendonitis, fatigue, muscle aches and pains, cramps, ankle sprains, and loss of muscular efficiency (reducing walking and running speed and endurance). The problems we see in the feet, which are due to over-pronation include bunions, heel spurs, plantar fasciitis, fallen and painful arches, hammertoes, metatarsalgia (ball of foot pain), and calluses. Diagnosis Look at the wear on your shoes and especially running trainers; if you overpronate it's likely the inside of your shoe will be worn down (or seem crushed if they're soft shoes) from the extra strain.  Non Surgical Treatment Over-Pronation can be treated conservatively (non-surgical treatments) with over-the-counter orthotics. These orthotics should be designed with appropriate arch support and medial rearfoot posting to prevent the over-pronation. Footwear should also be examined to ensure there is a proper fit. Footwear with a firm heel counter is often recommended for extra support and stability. Improper fitting footwear can lead to additional problems of the foot. Surgical Treatment The MBA implant is small titanium device that is inserted surgically into a small opening between the bones in the hind-mid foot: the talus (ankle bone) and the calcaneus (heel bone). The implant was developed to help restore the arch by acting as a mechanical block that prevents the foot from rolling-in (pronation). In the medical literature, the success rate for relief of pain is about 65-70%. Unfortunately, about 40% of people require surgical removal of the implant due to pain. Overview
During a growth spurt, your child?s heel bone grows faster than the muscles, tendons, and ligaments in her leg. In fact, the heel is one of your child?s first body parts to reach full adult size. When the muscles and tendons can?t grow fast enough to keep up, they are stretched too tight. If your child is very active, especially if she plays a sport that involves a lot of running and jumping on hard surfaces (such as soccer, basketball, or gymnastics), it can put extra strain on her already overstretched tendons. This leads to swelling and pain at the point where the tendons attach to the growing part of her heel. Causes Sever disease is more common in children who do regular sports or exercise that puts pressure on the heels. Activities such as running and jumping can put stress on the tight muscles and tendons. Symptoms Sever condition causes pain at the back of the heel. The pain is increased with plantar flexion of the ankle (pushing down with the foot as if stepping on the gas), particularly against resistance. Sever condition also causes tenderness and swelling in the area of the pain. Diagnosis A doctor or other health professional such as a physiotherapist can diagnose Sever?s disease by asking the young person to describe their symptoms and by conducting a physical examination. In some instances, an x-ray may be necessary to rule out other causes of heel pain, such as heel fractures. Sever?s disease does not show on an x-ray because the damage is in the cartilage. Non Surgical Treatment Treatment revolves around decreasing activity. Usual treatment has been putting children in a boot in slight equinus, or a cast with the foot in slight equinus, thereby decreasing the tension on the heel cord, which in turn pulls on the growth plate at the heel. As the pain resolves, children are allowed to go back to full activities. Complete resolution may be delayed until growth of the foot is complete (when the growth plate fuses to the rest of the bone of the heel). A soft cushioning heel raise is really important (this reduces the pull from the calf muscles on the growth plate and increases the shock absorption, so the growth plate is not knocked around as much). The use of an ice pack after activity for 20mins is often useful for calcaneal apophysitis, this should be repeated 2 to 3 times a day. As a pronated foot is common in children with this problem, a discussion regarding the use of long term foot orthotics may be important. If the symptoms are bad enough and are not responding to these measures, medication to help with inflammation may be needed. In some cases the lower limb may need to be put in a cast for 2-6 weeks to give it a good chance to heal. Surgical Treatment The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon. Overview
Many people have pain in the base of their foot. This could be due to overuse of one of many different structures in your foot. Common examples are sesamoiditis (inflammation of structures surrounding two small bones under the big toe joint) and plantar fasciitis (overuse of a ligament-like structure that runs underneath the length of the foot). Pain on standing first thing in the morning is a classic symptom of plantar fasciitis. It is one of the most common problems experienced by runners, accounting for about 10 per cent of running injuries. It is also common among middle-aged people, particularly if they are overweight. It often starts with low-grade pain in the arch or heel of the foot and can get worse over weeks or months.  Causes Flat feet are often hereditary. Arch pain may also be caused by wearing shoes with inadequate support, standing or walking for long periods of time in high heels, or overuse of the feet during work or sports. Being overweight also places additional stress on the feet, especially the arches. Symptoms Arch pain symptoms could include any of the following, a dull, constant ache if the ligaments have been stretched, swelling or tenderness in the foot, redness or bruising in the event of a more serious injury, difficulty putting weight on the foot, sharp pain when the foot is turned or manipulated, tenderness when pressure is applied. Because the arch of the foot is such a complex structure, arch pain could be an indicator of several different types of injuries. Chronic illnesses such as arthritis could also cause arch pain, and depending on the cause or source of your pain, you may experience discomfort in a variety of different areas. Ask a doctor if you believe you may have injured your foot arch. Diagnosis Magnetic Resonance Imaging (MRI) can show tendon injury and inflammation but cannot be relied on with 100% accuracy and confidence. The technique and skill of the radiologist in properly positioning the foot with the MRI beam are critical in demonstrating the sometimes obscure findings of tendon injury around the ankle. Magnetic Resonance Imaging (MRI) is expensive and is not necessary in most cases to diagnose posterior tibial tendon injury. Ultrasound has also been used in some cases to diagnose tendon injury, but this test again is usually not required to make the initial diagnosis. Non Surgical Treatment Rest from any aggravating activities and apply cold therapy whilst in the acute phase when the foot or ankle is painful and inflamed. Your Doctor may prescribe anti-inflammatory medication to help reduce pain and inflammation. Once the initial pain and inflammation has gone then a full rehabilitation program which includes stretching and strengthening exercises for the foot can begin. Consult a foot specialist, podiatrist or physiotherapist who can assess this and biomechanical problems of the foot. Nerve conduction studies may be done to confirm the diagnosis and indicate the location of the entrapment. An X-ray or MRI may also be useful to determine the presence of any other structures such as cysts, arthritis or a tarsal coalition.  Surgical Treatment A procedure that involves placing a metallic implant (most commonly) at the junction where the foot meets the ankle. This device causes the physical blockade that prevent the collapse. It is a procedure that is only indicated for mobile feet, and should not be used with rigid flat feet. Dr. Blitz finds this procedure better for younger patients with flexible flat feet where the bone alignment is still developing so that the foot can adapt to function in a better aligned position. Prevention Maintain a healthy weight, Use insoles to support your arches, Limit how often you wear high heels, Use proper shoes, especially when exercising to evenly distribute weight through your foot. Stretching Exercises Point your toes. To ease foot pain and aching in your feet, lift one foot and roll it downward until the toes are pointed toward the ground. Then flex your foot. Repeat using the other foot. This exercise will help stretch out all the small muscles that are on the bottom of your feet, which can help relieve aching and improve blood circulation. Raise your heels. This exercise is good for relieving toe cramps caused by standing for hours in constricting shoes, says Kurtz. Bonus: It can also strengthen calf muscles and make them look more defined. Stand up and lift your heels so that you are standing on the balls of your feet. Hold for 10 seconds. Repeat 10 times. Squeeze your toes. To strengthen the toes and help alleviate foot pain from hammertoes (when a toe resembles a claw), separate your toes using corks or foam toe separators and then squeeze your toes together for five seconds. Repeat 10 times. Roll a ball. Want to create an instant massage for the bottom of your feet? Roll a golf ball or tennis ball under the ball of your foot. Apply light pressure for about two minutes. This exercise can be helpful for arch pain, cramps, and heel pain from plantar fasciitis. Stretch standing up. A weight-bearing, runners-type stretch can be helpful for foot pain in the arch. Stand up and place your toes against a wall; lean forward a little until you feel your arch stretch. Repeat using the other foot. Stretch sitting down. Sit barefoot and cross your left leg so that your ankle rests on your right thigh. Then hold your toes and bend them back toward your shin, stretching the band of tissue connecting the bottom of the heel to the ball. A University of Rochester study found that people living with plantar fasciitis had a 75 percent chance of having no pain within three to six months of performing this stretch three times daily. Give yourself a foot massage. Nothing spells pain relief like a good foot rub. Use the following technique recommended by Rhonda Crockett, a licensed massage therapist at Ohio State University?s Center for Integrative Medicine in Columbus. Start with your toes, using your thumb to massage them in circular motions. Then move to the arch under your foot and gradually work your way down to the heel, applying pressure with your fingers and palm of your hand. Use lotion to allow your hand to move smoothly over your foot. Relax in a warm bath with Epsom salts. The combination of warm water and Epsom salts will give you a double dose of pain relief and relaxation. Magnesium sulfate, the key compound in Epsom salts, has been found to relax muscles, reduce pain, and sedate the nervous system. Plus, warm water helps improve circulation in the feet and relieve muscle pain. Crockett recommends adding two cups of Epsom salts to a warm bath and soaking for 20 minutes.
Overview
 Many of the muscles that move the foot are found in the lower leg. These muscles attach via tendons to various bones in the foot. The main muscles that move the foot downwards (plantar flex the foot) and propel the body forward are the calf muscles (gastrocnemius and soleus muscles). These muscles are connected to the heel bone (calcaneus) by the "rope like" Achilles tendon. Achilles tendon rupture is the term used to describe a complete tear of the Achilles tendon. The most common site for Achilles tendon rupture to occur is an area 2 - 6 cm. (1 - 2.5 in.) above where the tendon attaches to the calcaneus. Causes As with any muscle or tendon in the body, the Achilles tendon can be torn if there is a high force or stress on it. This can happen with activities which involve a forceful push off with the foot, for example, in football, running, basketball, diving, and tennis. The push off movement uses a strong contraction of the calf muscles which can stress the Achilles tendon too much. The Achilles tendon can also be damaged by injuries such as falls, if the foot is suddenly forced into an upward-pointing position, this movement stretches the tendon. Another possible injury is a deep cut at the back of the ankle, which might go into the tendon. Sometimes the Achilles tendon is weak, making it more prone to rupture. Factors that weaken the Achilles tendon are as follows. Corticosteroid medication (such as prednisolone) - mainly if it is used as long-term treatment rather than a short course. Corticosteroid injection near the Achilles tendon. Certain rare medical conditions, such as Cushing's syndrome, where the body makes too much of its own corticosteroid hormones. Increasing age. Tendonitis (inflammation) of the Achilles tendon. Other medical conditions which can make the tendon more prone to rupture; for example, rheumatoid arthritis, gout and systemic lupus erythematosus (SLE), lupus. Certain antibiotic medicines may slightly increase the risk of having an Achilles tendon rupture. These are the quinolone antibiotics such as ciprofloxacin and ofloxacin. The risk of having an Achilles tendon rupture with these antibiotics is actually very low, and mainly applies if you are also taking corticosteroid medication or are over the age of about 60. Symptoms When the Achilles tendon ruptures a loud bang or popping sound may be heard. The person may feel that they have been hit or kicked in the back of the lower leg and often they will look over their shoulder to see who or what has hit them. This is quickly followed by the sudden onset of sharp pain in the tendon and a loss of strength and function. If a complete rupture has occurred it may not be possible to lift the heel off the ground or point the toes. Often the degree of pain experienced, or lack of it, can be inversely proportional to the extent of the injury, ie a partial rupture may in fact be more painful than a complete rupture. Diagnosis Laboratory studies usually are not necessary in evaluating and diagnosing an Achilles tendon rupture or injury, although evaluation may help to rule out some of the other possibilities in the differential diagnosis. Plain radiography. Radiographs are more useful for ruling out other injuries than for ruling in Achilles tendon ruptures. Ultrasonography of the leg and thigh can help to evaluate the possibility of deep venous thrombosis and also can be used to rule out a Baker cyst, in experienced hands, ultrasonography can identify a ruptured Achilles tendon or the signs of tendinosis. Magnetic resonance imaging (MRI). MRI can facilitate definitive diagnosis of a disrupted tendon and can be used to distinguish between paratenonitis, tendinosis, and bursitis. Non Surgical Treatment Achilles tendon ruptures can be treated non-operatively or operatively. Both of these treatment approaches have advantages and disadvantages. In general, younger patients with no medical problems may tend to do better with operative treatment, whereas patients with significant medical problems or older age may be best served with non-operative treatment. However, the decision of how the Achilles tendon rupture is treated should be based on each individual patient after the advantages and disadvantages of both treatment options are reviewed. It is important to realize that while Achilles tendon ruptures can be treated either non-operatively or operatively, they must be treated. A neglected Achilles tendon rupture (i.e. one where the tendon ends are not kept opposed) will lead to marked problems of the leg in walking, which may eventually lead to other limb and joint problems. Furthermore, late reconstruction of non-treated Achilles tendon rupture is significantly more complex than timely treatment. Many of the muscles that move the foot are found in the lower leg. These muscles attach via tendons to various bones in the foot. The main muscles that move the foot downwards (plantar flex the foot) and propel the body forward are the calf muscles (gastrocnemius and soleus muscles). These muscles are connected to the heel bone (calcaneus) by the "rope like" Achilles tendon. Achilles tendon rupture is the term used to describe a complete tear of the Achilles tendon. The most common site for Achilles tendon rupture to occur is an area 2 - 6 cm. (1 - 2.5 in.) above where the tendon attaches to the calcaneus. Causes As with any muscle or tendon in the body, the Achilles tendon can be torn if there is a high force or stress on it. This can happen with activities which involve a forceful push off with the foot, for example, in football, running, basketball, diving, and tennis. The push off movement uses a strong contraction of the calf muscles which can stress the Achilles tendon too much. The Achilles tendon can also be damaged by injuries such as falls, if the foot is suddenly forced into an upward-pointing position, this movement stretches the tendon. Another possible injury is a deep cut at the back of the ankle, which might go into the tendon. Sometimes the Achilles tendon is weak, making it more prone to rupture. Factors that weaken the Achilles tendon are as follows. Corticosteroid medication (such as prednisolone) - mainly if it is used as long-term treatment rather than a short course. Corticosteroid injection near the Achilles tendon. Certain rare medical conditions, such as Cushing's syndrome, where the body makes too much of its own corticosteroid hormones. Increasing age. Tendonitis (inflammation) of the Achilles tendon. Other medical conditions which can make the tendon more prone to rupture; for example, rheumatoid arthritis, gout and systemic lupus erythematosus (SLE), lupus. Certain antibiotic medicines may slightly increase the risk of having an Achilles tendon rupture. These are the quinolone antibiotics such as ciprofloxacin and ofloxacin. The risk of having an Achilles tendon rupture with these antibiotics is actually very low, and mainly applies if you are also taking corticosteroid medication or are over the age of about 60. Symptoms When the Achilles tendon ruptures a loud bang or popping sound may be heard. The person may feel that they have been hit or kicked in the back of the lower leg and often they will look over their shoulder to see who or what has hit them. This is quickly followed by the sudden onset of sharp pain in the tendon and a loss of strength and function. If a complete rupture has occurred it may not be possible to lift the heel off the ground or point the toes. Often the degree of pain experienced, or lack of it, can be inversely proportional to the extent of the injury, ie a partial rupture may in fact be more painful than a complete rupture. Diagnosis Laboratory studies usually are not necessary in evaluating and diagnosing an Achilles tendon rupture or injury, although evaluation may help to rule out some of the other possibilities in the differential diagnosis. Plain radiography. Radiographs are more useful for ruling out other injuries than for ruling in Achilles tendon ruptures. Ultrasonography of the leg and thigh can help to evaluate the possibility of deep venous thrombosis and also can be used to rule out a Baker cyst, in experienced hands, ultrasonography can identify a ruptured Achilles tendon or the signs of tendinosis. Magnetic resonance imaging (MRI). MRI can facilitate definitive diagnosis of a disrupted tendon and can be used to distinguish between paratenonitis, tendinosis, and bursitis. Non Surgical Treatment Achilles tendon ruptures can be treated non-operatively or operatively. Both of these treatment approaches have advantages and disadvantages. In general, younger patients with no medical problems may tend to do better with operative treatment, whereas patients with significant medical problems or older age may be best served with non-operative treatment. However, the decision of how the Achilles tendon rupture is treated should be based on each individual patient after the advantages and disadvantages of both treatment options are reviewed. It is important to realize that while Achilles tendon ruptures can be treated either non-operatively or operatively, they must be treated. A neglected Achilles tendon rupture (i.e. one where the tendon ends are not kept opposed) will lead to marked problems of the leg in walking, which may eventually lead to other limb and joint problems. Furthermore, late reconstruction of non-treated Achilles tendon rupture is significantly more complex than timely treatment.  Surgical Treatment Debate remains regarding the best form of treatment for a ruptured Achilles tendon. The 2 options are:immobilisation or operation. A recent meta-analysis of scientific studies showed that compared to immobilisation, an operation reduces the risk of re-rupture and allows a quicker return to work. An operation is not without risk and these must be balanced against the benefit of a lower re-rupture rate. Both treatments involve immobilisation for 8 weeks. Prevention To help prevent an Achilles tendon injury, it is a good practice to perform stretching and warm-up exercises before any participating in any activities. Gradually increase the intensity and length of time of activity. Muscle conditioning may help to strengthen the muscles in the body. Surgical Treatment Debate remains regarding the best form of treatment for a ruptured Achilles tendon. The 2 options are:immobilisation or operation. A recent meta-analysis of scientific studies showed that compared to immobilisation, an operation reduces the risk of re-rupture and allows a quicker return to work. An operation is not without risk and these must be balanced against the benefit of a lower re-rupture rate. Both treatments involve immobilisation for 8 weeks. Prevention To help prevent an Achilles tendon injury, it is a good practice to perform stretching and warm-up exercises before any participating in any activities. Gradually increase the intensity and length of time of activity. Muscle conditioning may help to strengthen the muscles in the body.
Overview
 Feet usually have an arch on the inside portion of the foot. A flat foot is a foot that has lost or never developed this arch. It is often associated with the lower part of the legs being angled outwards. Most flat feet are flexible. This type rarely causes problems and usually do not require treatment. Rigid flat feet can cause problems and are best treated. Causes Some people develop fallen arches because they tend to pronate, or roll inwards on the ankles, says the Instep Foot Clinic. Other people may simply have under-developed muscles in their arches. Your arches help your feet bear weight and are supported in this job by muscles and tendons in your feet and ankles. So, while fallen arches aren?t usually serious, they can cause pain in your feet, ankles, knees and/or hips due to your reduced weight-bearing ability. In these cases, treatment may be required. Orthotics that sit in your shoes and support your arches are a common solution, as are exercises to strengthen and stretch your feet and leg muscles. Symptoms A significant number of people with fallen arches (flat feet) experience no pain and have no problems. Some, however, may experience pain in their feet, especially when the connecting ligaments and muscles are strained. The leg joints may also be affected, resulting in pain. If the ankles turn inwards because of flat feet the most likely affected areas will be the feet, ankles and knees. Some people have flat feet because of a developmental fault during childhood, while others may find that the problem develops as they age, or after a pregnancy. There are some simple devices which may prevent the complications of flat feet. Diagnosis If you notice that your feet are flat, but you?re not really experiencing any pain, then you?re probably okay to go without a visit to the podiatrist (unless, of course, you have a lack of feeling in your foot). You can schedule a hair appointment instead, or maybe see a movie. However, once painful symptoms start to appear, it?s better to skip the hirsute (or cinematic) experience and go see your foot doctor. Your podiatrist will likely make the diagnosis by examining your foot visually, asking about symptoms you may be experiencing, and may test your muscle strength. You may be asked to stand on your toes (in a ballerina pose, if you prefer, although that?s certainly not required), or walk around the examining room, and you may need to show the podiatrist your shoes. He or she may comment on your excellent taste in footwear, but is more likely to check your shoes for signs of wear that may indicate fallen arches. Your podiatrist may recommend X-rays, a CT scan or an MRI in order to get a look at the interior of your foot, although the best diagnosis usually comes from the doctor?s own in-person examination. Non Surgical Treatment Treatment often consists of giving the affected foot support from underneath so that the strain is taken off it (by the use of insoles or support pads) and so symptoms are relieved. A specialist in this problem is known as a podiatrist and these do work in the NHS - ask you father's doctor whether his condition is bad enough to warrant a referral to such a specialist. Surgical Treatment  Rarely does the physician use surgery to correct a foot that is congenitally flat, which typically does not cause pain. If the patient has a fallen arch that is painful, though, the foot and ankle physicians at Midwest Orthopaedics at Rush may perform surgery to reconstruct the tendon and "lift up" the fallen arch. This requires a combination of tendon re-routing procedures, ligament repairs, and bone cutting or fusion procedures. Prevention Well-fitted shoes with good arch support may help prevent flat feet. Maintaining a healthy weight may also lower wear and tear on the arches. Overview
 The common bunion is a localized area of enlargement of the inner portion of the joint at the base of the big toe. The enlargement actually represents a misalignment of the big toe joint (metatarsal phalangeal joint) and, in some cases, additional bone formation. The misalignment causes the big toe to point outward (medically termed hallux valgus deformity) toward the smaller toes. This deformity is progressive and will increase with time. The enlarged joint at the base of the big toe (the first metatarsophalangeal joint, or MTP joint) can become inflamed with redness, tenderness, and pain. A small fluid-filled sac (bursa) adjacent to the joint can also become inflamed (bursitis), leading to additional swelling, redness, and pain. A more deep joint pain may occur as localized arthritis develops in later stages of the deformity. A less common bunion is located at the joint at the base of the smallest (fifth) toe. This bunion is sometimes referred to as a tailor's bunion or bunionette. Causes Bunions are a common problem experienced mostly by women. The deformity can develop from an abnormality in foot function, or arthritis, but is more commonly caused by wearing improper fitting footwear. Tight, narrow dress shoes with a constrictive toe box (toe area) can cause the foot to begin to take the shape of the shoe, leading to the formation of a bunion. Women who have bunions normally wear dress shoes that are too small for their feet. Their toes are squeezed together in their shoes causing the first metatarsal bone to protrude on the side of the foot. It is important for men and women to realize that wearing dress shoes and boots, which are tapered in the toe area, can cause the bunion to worsen to the point where surgery is necessary. Symptoms A bony bump along the edge of the foot, at the base of the big toe (adjacent to the ball of the foot) Redness and some swelling at or near the big toe joint. Deep dull pain in the big toe joint. Dull achy pain in the big toe joint after walking or a sharp pain while walking. The big toe is overlapping the second toe, resulting in redness, calluses, or other irritations such as corns. Diagnosis Orthopaedic surgeons diagnose bunions on the basis of physical examination and weight bearing x-rays. Two angles are assessed, the intermetatarsal angle, that is between the first and second metatarsals (the bones that lead up to the base of the toes). If this angle exceeds 9? (the angle found in the healthy foot) it is abnormal and referred to as metatarsus primus varus. the hallux valgus angle, that is, the angle of the big toe as it drifts toward the small toe. An angle that exceeds 15? is considered to be a sign of pathology. Non Surgical Treatment Several things can be done to help relive the pain of bunions. These won't make the bunion go away, but they can make the foot more comfortable. Wearing different shoes. Shoes with a wide toe box rather than a pointed one will help. Shoes with lower heels will also help. (High heels throw more of the body's weight on the front part of the foot where the toe joints are.) Padding. Pads placed over the bunion may help reduce the pain. These are available from a drug store or may be available from a foot and ankle surgeon. Avoiding activities that make the pain worse. This includes standing for a long time or other activities that make the bunion sore. Non-steroidal anti-inflammatory drugs. These include aspirin or ibuprofen. They relieve pain and swelling. Applying an ice pack to reduce swelling and pain. Corticosteroid injections. These are not often used in bunion treatment. Injecting corticosteroids sometimes helps if the bursa is inflamed. (Bursa is a fluid-filled sac within a joint to cushion the bones). Orthotic devices. These are devices placed inside a shoe that shift the positioning of the foot. Orthotics help compensate for structural issues that cause foot problems. 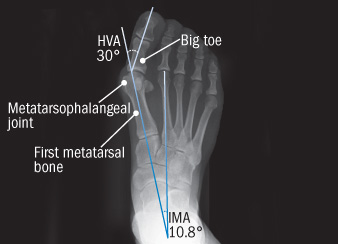 Surgical Treatment Severe cases may require, along with surgery, cast immobilization and prolonged avoidance of weight-bearing activity. You should know that undergoing surgery for this health problem does not guarantee a cure or even a beneficial health outcome. Bunions, like many other foot conditions, should always be approached from a prevention standpoint, or therapy should be directed at slowing the progression of your deformity. Overview
One of the most common causes of arch pain is plantar fasciitis, a condition that involves inflammation of the fibrous band of tissue that connects the heel to the toes (the plantar fascia). Pain from plantar fasciitis can be felt in the arch or the heel, and is most often felt toward the end of the day and after long periods of being stationary (e.g. getting up after sitting for a long time). Commonly, plantar fasciitis is the result of excessive foot pronation (rolling in of the foot) or excessive foot supination (e.g. high arches), both of which can increase tension on the plantar fascia. In these cases, orthotics and well-fitting footwear can address the cause of the problem by improving the position of the feet and relieving tension on the plantar fascia.  Causes Recent research has found a link with changes to the tendon in the foot and an increase in a type of protein called proteolytic enzyme. These enzymes can break down some areas of the tendon, weakening it and causing the foot arch to fall. Similar changes are also seen in other conditions, such as Achilles tendonitis. This could have important implications for treating flat feet because medication that specifically targets these enzymes could provide an alternative to surgery. However, further research is needed and this type of treatment is thought to be about 10 to 15 years away. Symptoms People suffering from pain in the arch sometimes complain of burning or soreness on the foot sole, which is worse in the morning and after physical activity. There may also be some tenderness when pressure is applied to the sole of the foot or heel. In addition to this, patients tend to complain of more pain when they stand on tiptoe. Diagnosis The doctor will take a brief history to determine how the injury occurred. If necessary, a thorough physical exam may be conducted to evaluate for any other injuries. Taking your workout shoes to the exam may also provide valuable information to the medical practitioner. Both feet will be physically and visually examined by the medical practitioner. The foot and arch will be touched and manipulated possibly with a lot of pressure and inspected to identify obvious deformities, tender spots, or any differences in the bones of the foot and arch. Non Surgical Treatment The most effective treatment for foot arch pain and strain is to use an arch support. The arch support sits under the foot and stops the arch of the foot from collapsing, thereby preventing the stretch of the arch pad which causes pain and discomfort. Wearing an arch support in slippers or house shoes can also prevent pain in the mornings when discomfort it most common and severe. Arch supports usually relieve symptoms within a few days.  Surgical Treatment In adults, the most common cause of collapse is due to the posterior tibial tendon tear. In such cases, the tendon must be repaired and a second tendon may be added to the posterior tibial tendon for strength and added support. If the foot is found to be very flat, bone realignment procedures or possible bone fusion procedures may be used to realign the foot. If the calf or Achilles tendon are found to be tight, they may be lengthened to allow better motion at the ankle and less arch strain. The forefoot may also be in a poor position and stabilization of the arch may be necessary to increase forefoot contact to the ground. Prevention The best way to prevent plantar fasciitis is to wear shoes that are well made and fit your feet. This is especially important when you exercise, walk a lot, or stand for a long time on hard surfaces. Get new athletic shoes before your old shoes stop supporting and cushioning your feet. You should also avoid repeated jarring to the heel. Maintain a healthy weight. Stretch when you feel a tightening of the ligament that runs along the bottom of your foot. Stop impact sports when symptoms first occur. |
AuthorWrite something about yourself. No need to be fancy, just an overview. ArchivesCategories |
 RSS Feed
RSS Feed
