|
Overview
 The common bunion is a localized area of enlargement of the inner portion of the joint at the base of the big toe. The enlargement actually represents a misalignment of the big toe joint (metatarsal phalangeal joint) and, in some cases, additional bone formation. The misalignment causes the big toe to point outward (medically termed hallux valgus deformity) toward the smaller toes. This deformity is progressive and will increase with time. The enlarged joint at the base of the big toe (the first metatarsophalangeal joint, or MTP joint) can become inflamed with redness, tenderness, and pain. A small fluid-filled sac (bursa) adjacent to the joint can also become inflamed (bursitis), leading to additional swelling, redness, and pain. A more deep joint pain may occur as localized arthritis develops in later stages of the deformity. A less common bunion is located at the joint at the base of the smallest (fifth) toe. This bunion is sometimes referred to as a tailor's bunion or bunionette. Causes Bunions are a common problem experienced mostly by women. The deformity can develop from an abnormality in foot function, or arthritis, but is more commonly caused by wearing improper fitting footwear. Tight, narrow dress shoes with a constrictive toe box (toe area) can cause the foot to begin to take the shape of the shoe, leading to the formation of a bunion. Women who have bunions normally wear dress shoes that are too small for their feet. Their toes are squeezed together in their shoes causing the first metatarsal bone to protrude on the side of the foot. It is important for men and women to realize that wearing dress shoes and boots, which are tapered in the toe area, can cause the bunion to worsen to the point where surgery is necessary. Symptoms A bony bump along the edge of the foot, at the base of the big toe (adjacent to the ball of the foot) Redness and some swelling at or near the big toe joint. Deep dull pain in the big toe joint. Dull achy pain in the big toe joint after walking or a sharp pain while walking. The big toe is overlapping the second toe, resulting in redness, calluses, or other irritations such as corns. Diagnosis Orthopaedic surgeons diagnose bunions on the basis of physical examination and weight bearing x-rays. Two angles are assessed, the intermetatarsal angle, that is between the first and second metatarsals (the bones that lead up to the base of the toes). If this angle exceeds 9? (the angle found in the healthy foot) it is abnormal and referred to as metatarsus primus varus. the hallux valgus angle, that is, the angle of the big toe as it drifts toward the small toe. An angle that exceeds 15? is considered to be a sign of pathology. Non Surgical Treatment Several things can be done to help relive the pain of bunions. These won't make the bunion go away, but they can make the foot more comfortable. Wearing different shoes. Shoes with a wide toe box rather than a pointed one will help. Shoes with lower heels will also help. (High heels throw more of the body's weight on the front part of the foot where the toe joints are.) Padding. Pads placed over the bunion may help reduce the pain. These are available from a drug store or may be available from a foot and ankle surgeon. Avoiding activities that make the pain worse. This includes standing for a long time or other activities that make the bunion sore. Non-steroidal anti-inflammatory drugs. These include aspirin or ibuprofen. They relieve pain and swelling. Applying an ice pack to reduce swelling and pain. Corticosteroid injections. These are not often used in bunion treatment. Injecting corticosteroids sometimes helps if the bursa is inflamed. (Bursa is a fluid-filled sac within a joint to cushion the bones). Orthotic devices. These are devices placed inside a shoe that shift the positioning of the foot. Orthotics help compensate for structural issues that cause foot problems. 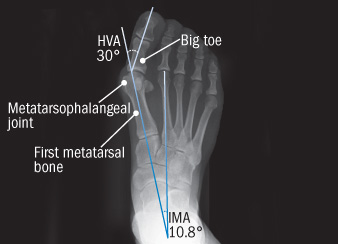 Surgical Treatment Severe cases may require, along with surgery, cast immobilization and prolonged avoidance of weight-bearing activity. You should know that undergoing surgery for this health problem does not guarantee a cure or even a beneficial health outcome. Bunions, like many other foot conditions, should always be approached from a prevention standpoint, or therapy should be directed at slowing the progression of your deformity. Overview
One of the most common causes of arch pain is plantar fasciitis, a condition that involves inflammation of the fibrous band of tissue that connects the heel to the toes (the plantar fascia). Pain from plantar fasciitis can be felt in the arch or the heel, and is most often felt toward the end of the day and after long periods of being stationary (e.g. getting up after sitting for a long time). Commonly, plantar fasciitis is the result of excessive foot pronation (rolling in of the foot) or excessive foot supination (e.g. high arches), both of which can increase tension on the plantar fascia. In these cases, orthotics and well-fitting footwear can address the cause of the problem by improving the position of the feet and relieving tension on the plantar fascia.  Causes Recent research has found a link with changes to the tendon in the foot and an increase in a type of protein called proteolytic enzyme. These enzymes can break down some areas of the tendon, weakening it and causing the foot arch to fall. Similar changes are also seen in other conditions, such as Achilles tendonitis. This could have important implications for treating flat feet because medication that specifically targets these enzymes could provide an alternative to surgery. However, further research is needed and this type of treatment is thought to be about 10 to 15 years away. Symptoms People suffering from pain in the arch sometimes complain of burning or soreness on the foot sole, which is worse in the morning and after physical activity. There may also be some tenderness when pressure is applied to the sole of the foot or heel. In addition to this, patients tend to complain of more pain when they stand on tiptoe. Diagnosis The doctor will take a brief history to determine how the injury occurred. If necessary, a thorough physical exam may be conducted to evaluate for any other injuries. Taking your workout shoes to the exam may also provide valuable information to the medical practitioner. Both feet will be physically and visually examined by the medical practitioner. The foot and arch will be touched and manipulated possibly with a lot of pressure and inspected to identify obvious deformities, tender spots, or any differences in the bones of the foot and arch. Non Surgical Treatment The most effective treatment for foot arch pain and strain is to use an arch support. The arch support sits under the foot and stops the arch of the foot from collapsing, thereby preventing the stretch of the arch pad which causes pain and discomfort. Wearing an arch support in slippers or house shoes can also prevent pain in the mornings when discomfort it most common and severe. Arch supports usually relieve symptoms within a few days.  Surgical Treatment In adults, the most common cause of collapse is due to the posterior tibial tendon tear. In such cases, the tendon must be repaired and a second tendon may be added to the posterior tibial tendon for strength and added support. If the foot is found to be very flat, bone realignment procedures or possible bone fusion procedures may be used to realign the foot. If the calf or Achilles tendon are found to be tight, they may be lengthened to allow better motion at the ankle and less arch strain. The forefoot may also be in a poor position and stabilization of the arch may be necessary to increase forefoot contact to the ground. Prevention The best way to prevent plantar fasciitis is to wear shoes that are well made and fit your feet. This is especially important when you exercise, walk a lot, or stand for a long time on hard surfaces. Get new athletic shoes before your old shoes stop supporting and cushioning your feet. You should also avoid repeated jarring to the heel. Maintain a healthy weight. Stretch when you feel a tightening of the ligament that runs along the bottom of your foot. Stop impact sports when symptoms first occur.
Overview
 The Achilles tendon is the thickest and strongest tendon in the human body. It plays a very important role in most sport activities and is particularly vulnerable to overloading from repetitive running and jumping. The Achilles tendon forms a joint distal tendon for the gastrocnemius and the soleus muscles. These muscles combine to form the triceps surae muscle. Athletes who sustain Achilles tendon ruptures most frequently are those who participate in ball sports that demand rapid changes of direction and quick, reactive jumps (e.g., tennis, squash, badminton, and soccer), in addition to runners and jumpers in track and field. Sometimes a patient with a ruptured tendon has a history of long-term pain localized to the tendon, but more often the rupture occurs without warning. Such ruptures are often caused by degenerative changes in the tendon (tendinosis), usually in the segment of the tendon that has the worst blood supply. This segment extends from 2 to 6 cm proximal to the insertion of the tendon onto the calcaneus. The Achilles tendon is the thickest and strongest tendon in the human body. It plays a very important role in most sport activities and is particularly vulnerable to overloading from repetitive running and jumping. The Achilles tendon forms a joint distal tendon for the gastrocnemius and the soleus muscles. These muscles combine to form the triceps surae muscle. Athletes who sustain Achilles tendon ruptures most frequently are those who participate in ball sports that demand rapid changes of direction and quick, reactive jumps (e.g., tennis, squash, badminton, and soccer), in addition to runners and jumpers in track and field. Sometimes a patient with a ruptured tendon has a history of long-term pain localized to the tendon, but more often the rupture occurs without warning. Such ruptures are often caused by degenerative changes in the tendon (tendinosis), usually in the segment of the tendon that has the worst blood supply. This segment extends from 2 to 6 cm proximal to the insertion of the tendon onto the calcaneus.Causes Ruptured Achilles tendons may result from falling from a height or down a hole. Increasing training intensity abruptly, boosting distance, frequency or duration by more than 10% a week. Failing to stretch before and after exercise. Repetitive training, especially uphill running. Deyhydration, which causes cramping and tightness in the calves. Taking antibiotics. Improper footwear. Explosive movements in competitive sports like basketball, soccer or track & field. Symptoms If the Achilles tendon is ruptured you may experience a sudden pain in the back of your leg, as if someone had kicked you, followed by, swelling, stiffness, and difficulty to stand on tiptoe and push the leg when walking. A popping or snapping sound may be heard when the injury occurs. You may also feel a gap or depression in the tendon, just above heel bone. Ruptures usually occurs in those aged 30 - 70 years, during a sudden forceful push off from the foot. Without proper healing of the tendon, you will have a permanent limp and weakness when using the leg. Diagnosis Other less serious causes of pain in the back of the lower leg include Achilles tendonitis or bursitis. To distinguish between these possibilities, your physician will take a thorough history and examine your lower leg to look for signs of a rupture. The presence of a defect in the tendon that can be felt, evidence of weakness with plantarflexion, and a history consistent with Achilles tendon rupture are usually sufficient for diagnosis. Your physician may also perform a Thompson test, which consists of squeezing the calf muscles of the affected leg. With an intact Achilles tendon, the foot will bend downward; however, with a complete rupture of the tendon, the foot will not move. In cases where the diagnosis is equivocal, your physician may order an MRI of the leg to diagnose a rupture of the Achilles tendon. Non Surgical Treatment Nonsurgical treatment involves extended casting, special braces, orthotics, and physical therapy. Avoids the normal complications and expenses of surgery. Some studies show the outcome is similar to surgery in regard to strength and function. There is risk of an over-lengthened tendon with inadequate tension. Extended immobilization can lead to more muscle weakness. Nonsurgical treatment has a higher incidence of re-rupture than surgical repair. Nonsurgical treatment is often used for nonathletes or for those with a general low level of physical activity who would not benefit from surgery. The elderly and those with complicating medical conditions should also consider conservative nonsurgical treatment.  Surgical Treatment Referral to a surgeon for open or percutaneous repair of the tendon is often necessary, followed by an immobilisation period. Functional bracing and early mobilisation are becoming more widely used postoperatively. There is no definitive protocol for this and it may differ, depending on the surgeon. Operative treatment has a reduced chance of re-rupture compared with conservative treatment (3.5% versus 12.6%) and a higher percentage of patients returning to the same level of sporting activity (57% versus 29%). The patient's desired functional outcome and comorbidities that affect healing will be factors in the decision to operate. |
AuthorWrite something about yourself. No need to be fancy, just an overview. ArchivesCategories |
 RSS Feed
RSS Feed
